
 Figure 1. (Click to enlarge) |
A 46-year-old woman presents to the emergency department (ED) with a history of worsening, constant right upper quadrant pain that radiates to her back and side. She has had nausea and has vomited twice in the past several hours. The intake triage nurse considers that she may have ingested something toxic, and turns immediately to her Emergency Physician who is also a well known toxicology expert consultant. But he learns upon questioning that she underwent a laparoscopic cholecystectomy 2 weeks ago, without complications, and returned to her normal diet. She has not had any bowel movements or flatulence since the pain began. She denies having any fever, chills, or rigors. Her medical history is significant only for high blood pressure, high cholesterol levels, and gallbladder disease. She takes lisinopril, aspirin, multivitamins, and ginseng. She denies smoking or drinking alcohol.
On physical examination, the patient is awake, alert, and oriented. Her vital signs are within the normal range, with a heart rate of 84 bpm and a blood pressure of 124/76 mm Hg. She appears to be in mild distress. The cardiorespiratory examination yields normal findings, with clear lungs and a regular heart rhythm. Her abdomen is soft, but her bowel sounds are decreased, and she has marked tenderness in the right upper quadrant. The rest of her abdomen is minimally tender, with no evidence of guarding or rebound and no palpable masses. The other physical findings are normal.
The laboratory investigation reveals an elevated WBC count of 14.0 × 109/L (14.0 × 103/µL), with a left shift of 87% neutrophils. Her liver function tests, lipase level, and basic chemistry panel are unremarkable.
Contrast-enhanced computed tomography (CT) scans of the abdomen and pelvis are ordered. Figure 1A shows an anteroposterior (AP) scout image, and Figure 1B shows a selected axial section. The appearance of the xrays is that of bean-like substances.
The diagnosis is Cecal Volvulus.
Discussion
The initial scout image (see Figure 2A) demonstrates a markedly dilated segment of bowel with a "kidney-bean" appearance. The vector of the C-loop points toward the right lower quadrant and suggests a cecal volvulus. The axial CT image (see Figure 2B) demonstrates a colon dilated to 8 cm, with an air-fluid level. The collapsed ascending colon and transverse colon are adjacent to the dilated bowel (arrow).
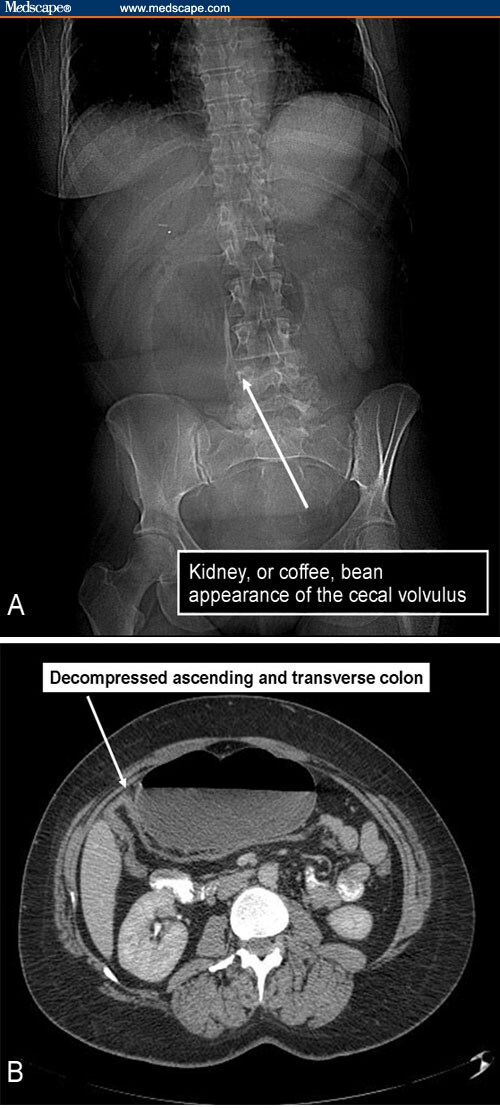 Figure 2. (Click to enlarge) |
Cecal volvulus is a condition that is characterized by twisting or folding of the right colon. The term cecal volvulus is actually a misnomer because, in most patients with cecal volvulus, the torsion is located in the ascending colon above the ileocecal valve. In general, a partial malrotation is necessary for cecal volvulus to occur because, besides the cecum, parts of the ascending colon are also involved. Defective peritoneal fixation of the ascending colon and cecum has been described in approximately 10% of the population; because this defective fixation results in abnormal mobility of the ascending colon and cecum, displacement of the right colon into any part of the abdominal cavity is possible. An association with adhesions, membranes, and bands, which may provide a nodal point around which the mobile ascending colon may twist, has been described; although these conditions are frequently present, they are not required for a volvulus to occur. Other predisposing risk factors with clearly defined roles in the development of cecal volvulus have also been described. Associations with colonic atony, partial distal large-bowel obstruction, traction resulting from disease of the appendix, colonoscopy, pregnancy, postoperative abdomen, and colonic ileus (pseudo-obstruction) have all been reported. The most common distal colonic lesions associated with cecal volvulus are colonic carcinoma and diverticulitis. Urticaria, with submucosal edema and cellular infiltrate of the bowel, has also been reported in association with cecal volvulus.
Two types of cecal volvulus are described: cecal bascule (type 1; which accounts for approximately 10% of cases) and axial torsion (type 2; which accounts for approximately 90% of cases). Axial torsion, or type 2, occurs when the ascending colon twists 180-360° along its longitudinal axis. Type 2 cecal volvulus is associated with a high mortality rate because of the resultant vascular compromise, which can lead to gangrene and perforation. In the cecal bascule type of volvulus, the cecum folds anteromedially to the ascending colon. A flap-valve occlusion at the site of flexion develops, with marked distention of the cecum and central displacement. Reduction of a cecal bascule after a barium enema has been reported. The ileum may passively twist with the cecum, and usually, a constricting band across the ascending colon is present, which is found at laparotomy.
Volvulus of the large bowel is the cause of approximately 10% of large-bowel obstructions. Cecal volvulus represents approximately 1-2% of intestinal obstructions and about 33% of all cases of colonic volvulus. The majority of volvulus cases are caused by sigmoid volvulus. Cecal volvulus occurs predominantly in patients with poor right colon fixation (found in 10-25% of the general population) and is caused by excessive cecal mobility.
Patients with cecal volvulus usually present with an acute onset of severe, colicky pain with nausea and vomiting, unless partial obstruction is present or the volvulus is intermittent; in the latter cases, the onset may be relatively insidious. Abdominal distention may or may not develop. Proposed etiologies for cecal volvulus include trauma, laxative use, appendicitis, postoperative complications (such as adhesions), constipation, postpartum ligamentous laxity, and distal colonic obstruction from colon cancer or diverticulitis. Cecal volvulus may also occur in other clinical situations, such as after a colonoscopy or a barium enema study, as well as in pregnancy.
An abdominal series alone will help make the diagnosis in approximately 50% of cases of cecal volvulus. The radiographs show a single air-fluid level in a dilated, air-filled cecum in the midabdomen or in the left upper quadrant. The cecal valve may produce a soft-tissue indentation, creating a "kidney-bean" appearance to the air-filled cecum; this is in contrast to a "coffee-bean" sign, caused by grossly dilated and closely apposed loops of bowel, which is more typically noted with sigmoid volvulus. The small bowel should be dilated or fluid-filled, unless the process is early in its course and the bowel has collapsed. In axial torsion, the radiograph may show a markedly distended loop of large bowel with its long axis extending from the right lower quadrant to the epigastrium or the left upper quadrant; this is the most common site to which the cecum is displaced. If the obstruction is complete, the distal colon is usually empty and, frequently, the small bowel is distended. In the cecal bascule form of volvulus, the distended air-filled cecum is more centrally located. With this variant, the ileum can passively twist with the cecum, and the small bowel may not be obstructed. If abdominal radiographs are nondiagnostic, CT scanning or contrast enema studies can help to further define the condition. Barium enema studies can show beaking at the point of the volvulus in the mid-ascending colon. CT scans show the volvulus itself and progressive tapering of the afferent and efferent limbs, which leads to a twist; this is described as the whirl sign. Ultrasonography, if used to investigate the acute abdomen, may demonstrate the small-bowel loops of an associated small-bowel obstruction, or the cecal volvulus may appear as a grossly distended fluid-filled cecum at a lead point of small-bowel obstruction, but generally, the appearances are nonspecific.
Treatment usually consists of surgical reduction with or without a colonic resection and an ileocolostomy. Nonsurgical techniques, such as barium enemas and colonoscopy, are less successful for reducing cecal volvulus than for sigmoid volvulus, and the rate of associated perforation is higher with a cecal volvulus than it is with a sigmoid volvulus. Nonsurgical reduction may be most successful in type 1 volvulus (cecal bascule). Although treatment and management is the same for type 1 and type 2, a type 2 volvulus increases the risk of vascular compromise and perforation. Perforation occurs in 65% of cases involving mechanical distention combined with a vascular compromise. Gangrene is observed in as many as 20% of patients, and mortality is estimated to be as high as 20-40% in the elderly.
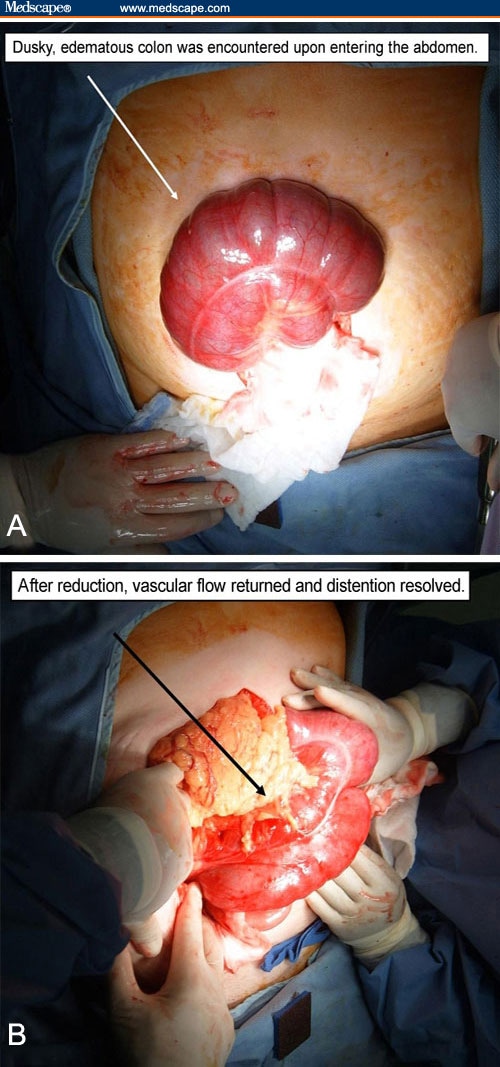 Figure 3. (Click to enlarge) |
The patient underwent an exploratory laparotomy for the bowel obstruction and the suspected cecal volvulus, without a preoperative attempt at reduction. The cecum was edematous and exhibited a dusky appearance (see Figure 3A). A floppy segment of bowel that was not adherent to the lateral wall had folded upward into the upper abdomen and twisted around; these observations were consistent with the final diagnosis of cecal volvulus. The volvulus was reduced, and the color of the involved bowel improved ("pinked up") nicely (see Figure 3B). A right colonic resection was performed with a stapled ileocolostomy, without complication; this was done because of a risk of recurrence and the possibility of underlying ischemic damage (even though flow may have been restored). The pathology screening revealed ischemic changes, with marked dilatation and serosal adhesions; no perforation was observed. The patient recovered uneventfully.
Case Study from eMedicine February 27, 2008